

Japanese Encephalitis
What Is Japanese Encephalitis?


Japanese Encephalitis (JE) is a viral disease spread by mosquitoes from infected animals (usually pigs and wading birds) to humans. Since the mosquito that carries the virus breeds in flooded rice fields and pools of water, most human infections occur in rural, agricultural areas in Asia (although occasional cases have been reported from urban locations). About 50,000 cases are reported each year in Asia, however only a small number of cases have occurred in travellers.
What Are The Symptoms Of Japanese Encephalitis?
In its early stages, Japanese Encephalitis presents with a flu-like illness with headache, fever, gastrointestinal symptoms, confusion and other behaviour disturbances. If the illness progresses to inflammation of the brain, up to 30% of cases end in death and half end in permanent disability. There is currently no effective drug treatment for the disease once it sets in – it can only run its course. Nevertheless, it is very important to seek supportive medical treatment.
Who Is At Risk?

The risk to short-term travellers and those who confine their travel to urban centres is very low. Expatriates and travellers living for prolonged periods in rural areas where Japanese Encephalitis is endemic or epidemic are at greatest risk. People with extensive unprotected outdoor, evening and night time exposure in rural areas, such as travellers who are bicycling, camping, or engaging in certain occupational activities, might be at high risk even if their trip is brief. Lab workers for whom exposure to JE virus is possible should also consider vaccination. Travellers over 55 who are going to risk areas during the transmission season should give special consideration to receiving the vaccine as they are more likely to develop permanent disability. Pregnant women should discuss with their physicians the advisability of travel to risk areas during transmission seasons, as infection during the first and second trimesters is associated with intrauterine infection and miscarriage.
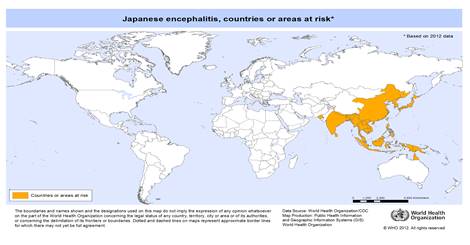
In What Areas Of The World Does Japanese Encephalitis Occur?

The main risk areas are in China, the Korean peninsula, the Indian subcontinent and SE Asia. Major epidemics have occurred in the past in China, Korea, Japan, Taiwan and Thailand. Periodic epidemics continue to occur in Vietnam, Cambodia, Myanmar, Laos, India, Nepal, the Philippines and Malaysia. JE has occurred in lower frequency in Singapore, Hong Kong, Eastern Russia, Guam, Saipan, Brunei and the Torres Strait Islands.
Transmission tends to occur seasonally in most areas of Asia. In temperate regions, the transmission season generally extends from May through September. In tropical and subtropical regions, transmission is typically greatest during the rainy season and early dry season (which varies by region). In some areas, however, irrigation may cause transmission to occur throughout the year. Areas above 1500 metres and urban areas are generally low risk.
How Can I Prevent It?
Every traveller's first line of defence is to take personal protective measures against mosquitoes. There is a risk of contracting other mosquito-borne illnesses in Asia. The mosquitoes that transmit Japanese Encephalitis feed mainly outdoors during the cooler hours at dusk and dawn. Avoid being outdoors during these times, wear mosquito repellent containing DEET, stay in air-conditioned or well-screened rooms and use aerosol insecticides and mosquito coils as necessary. Reduce your amount of skin exposure by wearing socks, long pants and long-sleeved shirts. If you will be travelling in rural areas, carry along a portable bednet which can be impregnated with permethrin (clothing can also be impregnated), both of which are available from our clinic.
Vaccination
There are currently 2 vaccines available in Australia;
- IMOJEV is a single vaccine that provides cover for a minimum of 4 years. With this vaccine, caution must be taken when administering with other vaccines at the same time, as it is a live vaccine. Recommended to be given 28 days before departure. Available for adults and children from the age of 12 months and over.
- JESPECT is a course 2 vaccines of an inactivated viral vaccine, given 28 days apart. Recommended to be given at least 35 days before departure. Long- term residents in risk areas should consider a booster 15 months after the primary course. Available for adults and children from 2 months of age onwards.
Risks and Side Effects: Reactions are usually mild and go away within a few days. Approximately 40% of people experience reactions including pain, redness, and swelling at the injection site. The most common reactions include headache (about 20%) and muscle pain (about 13%). As with any vaccine, there is a very small risk of anaphylaxis.
Who Should Not Have The Vaccine?
As a general rule, some people should not be vaccinated unless the benefit of the vaccine clearly outweighs the disease risk:
- Children less than 2 months of age.
- Pregnant or breastfeeding women, unless at substantial risk of JE exposure.
- Anyone with a moderate or severe illness
Updated August 2021.